As much as medicine desires to be a purely objective science, it is still mired in ethical controversy as a consequence of its human element. Often, medical decisions are not always made through logical reasoning, but rather include social, emotional, and economical components, among others. However, what ties together these alternate components is the rhetorical discourse between the patient and physician, patient and family, and more generally, the patient and society at large.
In order to effectively work within this rhetorical environment, physicians should realize that medicine inherently lies at the intersection of art and science. In some ways, it is the perfect blend of creativity, technique, empathy, emotion, technology, and evidence-driven science. However, medicine remains first and foremost an applied science, and therefore it must contend with the divergent goals of not only serving the needs of the patient but also furthering the scientific study of the human body. Whether or not medicine is able to reconcile these discordant ambitions is a complex issue. However, the conflict is particularly evident in end of life care. Medicine has continuously struggled to answer the question: at what point do physicians, or the patients for that matter, decide that enough is enough? When is intensive medical care considered to too costly (both in terms of the wellbeing of the patient, as well as more recently the monetary expense)? This questions is often posed to patients and physicians alike during difficult times, for example, when patients are facing a terminal illness, or are unresponsive and on the brink of death. What role does medicine play, or rather what role should it play when there is nothing more that can be done? What role should medicine play when what can be done in fact causes more harm?
The answer to this question has changed drastically within the last two decades during which the pace of advancement has exponentially increased. Some might even argue that medicine has advanced past the point of “naturality,” or in other words, to the point of being able to artificially support life for longer than considered natural. At the same time, the majority of Americans have expressed the desire for a peaceful death, free of pain and unnecessary intensive care. As the aggregation of discourses surrounding this topic has evolved, public policy has adapted to reflect that desire, with the establishment of advanced directives and the “Do Not Resuscitate” order. Although beneficial in reducing unwanted intensive care, this idea has had its share of controversy, particularly when a patient reverses their decision when faced with death and decides that they do, in fact, wish to be resuscitated at the last minute.
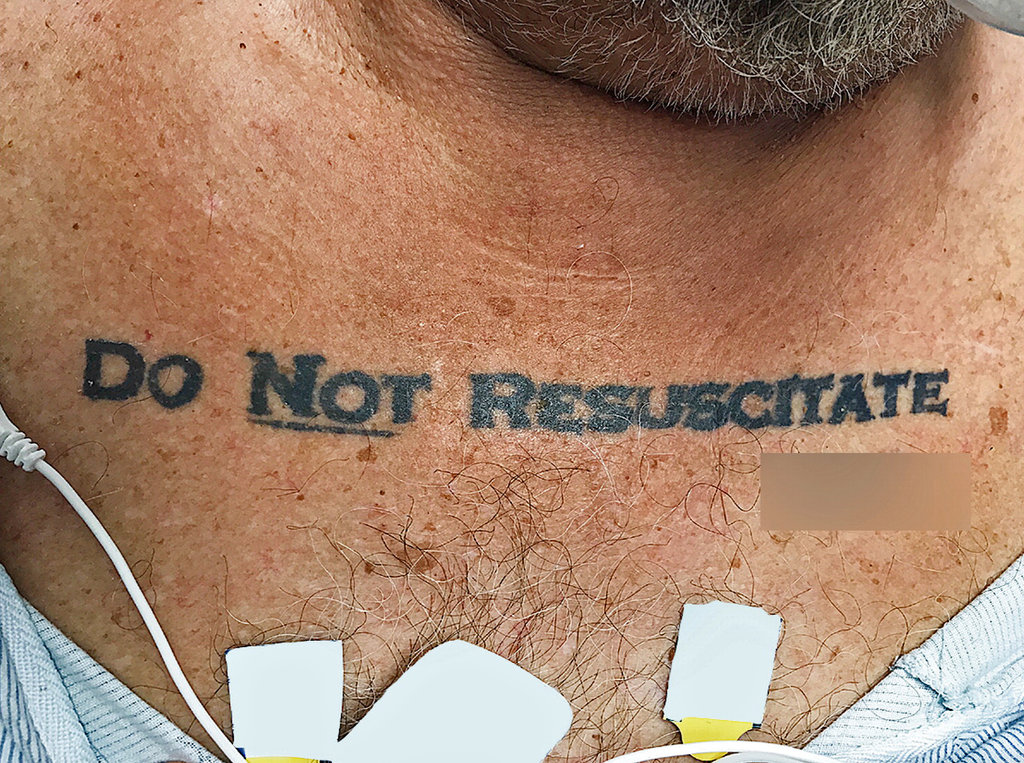
As a result, effective communication of the patient’s end-of-life desires are critical. This communication issue is exacerbated when the patient is not able to express their wishes directly, and this has real life ramifications. Emergency physicians were confronted with a difficult dilemma when an unresponsive and deteriorating 70 year old male patient was brought to the emergency department. He had a tattoo on his chest with the words “Do Not Resuscitate” in bold lettering, followed by a signature, as shown in Figure 1. This situation, although ostensibly a medical ethics issue, is in fact inherently rhetorical in nature.

Fig. 1 – Photograph of patient’s “Do Not Resuscitate” tattoo on the chest (Image: Holt, NEJM)
The attending physicians struggled to make a decision in discerning whether or not the tattoo was an accurate representation of the patient’s wishes and whether or not it was legally valid without the presence of an official state-sponsored document. Eventually the physicians decided to not honor the tattoo, “invoking the principle of not choosing an irreversible path when faced with uncertainty” (Holt, 2017). This is the aggregation of discourses at act; the medical field has decided that life saving interventions is the default mode of action. In essence, the discourses contend that life is too precious to lose, almost regardless of cost, even if the cost is to the patients themselves. The question becomes, does the tattoo represent the true desires of the patient, or is it a regrettable attempt at morbid humor? If the patient were conscious, would he request doctors to ignore the tattoo?
Rhetorically, tattoos hold little significance in comparison to other forms of communication. However, this begs the question, why would doctors choose to ignore the tattoo? Why is the tattoo considered an inadequate form of communication? The general negative stigma surrounding tattoos is likely a significant contributor. Some tattoos serve as permanent reminders of a regrettable decisions while a person was intoxicated. The possibility that the patient did not intend the tattoo to be taken seriously forced the physicians to err on the side of caution. Despite this, the attending physicians remarked that “this decision left us conflicted owing to the patient’s extraordinary effort to make his presumed advance directive known” (Holt, 2017). This conflict led to the physicians requesting an ethics consultation.
Following careful review the ethics committee advised the physicians to honor the wishes of the patient’s tattoo. They argued that “it was most reasonable to infer that the tattoo expressed an authentic preference, that what might be seen as caution could also be seen as standing on ceremony, and that the law is sometimes not nimble enough to support patient-centered care and respect for patients’ best interests” (Holt, 2017). The process of obtaining a D.N.R. order can be challenging and time-consuming, and therefore patients may eventually choose to take matters into their own hands.
Despite being given exactly the same data, i.e. a terminally ill and deteriorating patient with a “Do Not Resuscitate” tattoo, the physicians and ethics committee made differing claims. This is attributed to the different warrants used to justify the claims. Specifically, the physicians used their professional “gaze” in order to establish a warrant that they have a responsibility in prolonging life to the best of their ability, as well as the discourses within the physician community as justification. However, the warrant of the ethicists relies much more strongly upon the relatively new idea of patient-centered care with respect to end-of-life directives and the notion that medical intervention may not necessarily be in the best interest of the patient. Importantly, a warrant common to both the physicians and the ethicists is that the tattoo may not reflect the current desires of the patient, given its permanency in contrast with the much more malleable nature of human ideology.
Would the ethicists have made the same decision, however, had the patient not been in deteriorating condition? Would they have instead waited until the patient became conscious, albeit potentially in significant pain, to confirm their desires? This alludes to the fact that rhetoric is highly contextual; that is, contextual clues can often change the meaning and seriousness of the message. Just as human perception forces a reality to be constructed spontaneously “on the fly,” the rhetorical situation is itself built on that perception and is therefore processual as well. At each situation, the rhetorical perception is reconstructed based on the aggregation of discourses that existed prior, and most importantly, those discourses are constantly added to and modified as the environment changes. Thus the discourses are alway in flux, slowly adapting alongside society.
Currently, when an unresponsive patient presents with a life threatening illness, the general presumption—that is, the current aggregation of discourses in the medical field—is to care for the patient and prevent death to the best of medical practitioner’s ability. This is an aggregation of discourses that has roots in society’s fear of death. However, this discourse is slowly changing in response to the acute realization that death, and specifically a pain-free death, is not always unwelcome.
Of note is that, subsequent to the decision by the ethical committee, the social work department was able to identify the patient and obtain the patient’s official Florida DNR order, “which was consistent with the tattoo” (Holt, 2017). The patient continued to deteriorate and eventually passed away without further advanced airway management. The attending physicians note that they “were relieved to find his written DNR request, especially because a review of the literature identified an earlier case report of a person whose DNR tattoo did not reflect his current wishes” (Holt, 2017). This earlier case provides an antithesis to the argument that the tattoo accurately reflected the patient’s desire that his end-of-life wishes be conveyed appropriately and taken seriously.
A few years earlier, a 59 year old man with diabetes presented to the hospital with a “D.N.R.” tattoo on his chest, shown in Figure 2. However, this patient explained that though he did not want prolonged attempts at life saving care, “he indicated that he would want resuscitative efforts in the event of cardiac or respiratory arrest” (Cooper, 2012). The patient later explained to physicians that he had lost a bet and consequently had to tattoo “D.N.R” on his chest. “He stated that he did not think anyone would take his tattoo seriously and declined tattoo removal” (Cooper 2012).

Fig. 2 – Photograph of patient’s tattoo that was regretted (Image: Cooper, JGIM)
In context of these situations, the rhetorical implications of a “Do Not Resuscitate” tattoo have serious consequences for patients and their families, as well as for the field of medicine as a whole. However, in each case, a rhetorical analysis is completed based on the aggregation of discourses at the time, which is continually being modified and updated to reflect a changing society, and its changing values.
References
Bever L. A man collapsed with ‘Do Not Resuscitate’ tattooed on his chest. Doctors didn’t know what to do. Washington Post. December 1, 2017. https://www.washingtonpost.com/news/to-your-health/wp/2017/12/01/a-man-collapsed-with-do-not-resuscitate-tattooed-on-his-chest-doctors-didnt-know-what-to-do/. Accessed February 2, 2018.
Cooper L, Aronowitz P. DNR Tattoos: A Cautionary Tale. Journal of General Internal Medicine. 2012; 27(10):1383-1383. doi:10.1007/s11606-012-2059-8.
Fortin J. His Tattoo Said ‘Do Not Resuscitate.’ Doctors Wanted Another Opinion. New York Times. December 4, 2017. https://www.nytimes.com/2017/12/04/us/do-not-resuscitate-tattoo.html. Accessed February 2, 2018.
Holt GE, Sarmento B, Kett D, Goodman KW. An Unconscious Patient with a DNR Tattoo. New England Journal of Medicine. 2017; 377(22):2192-2193. doi:10.1056/nejmc1713344.
Khullar D. We’re Bad at Death. Can We Talk? New York Times. May 10, 2017. https://www.nytimes.com/2017/05/10/upshot/were-bad-at-death-first-we-need-a-good-talk.html. Accessed February 2, 2018.