
The only red in the operating room was the digital clock on the back wall, blinking steadily above the C-arm tucked neatly beside the anesthesia workstation. “Tourniquet time, six forty-two a.m.,” Alia Brooks croaked as she sat down on the stool. She was the second-year orthopedic resident on call last night and had slept in the call room for a blissful four and a half hours before this, the first case of the day. She wasn’t sure how Saanen would react if she said her thoughts out loud. Would he page the other resident, or would he tell her to suck it up and get used to the lack of sleep? She hadn’t done many scaphoid ORIFs before.
Dr. Errol Saanen stood across the hand table, with perfect posture. His lean figure belied the tension in his muscles. When Alia first met him at a research conference in med school, she would never have guessed that the poised man would appear so lanky in scrubs and lead. He was the only one in the room completely at ease. Alia wiggled her fingers, trying to get the blood flowing, yet she couldn’t get them to feel any less cold or stiff under the gloves. Despite changing into new scrubs before rounds at 6 a.m., she felt her sweat seeping into the fabric. Her warm breath escaped her mask with each exhalation, jetting upward right at her eyelashes. At least she wasn’t having a migraine today, probably a result of the two ibuprofen tablets she snuck in with her burnt coffee.
Between Alia and Saanen, the patient’s left arm lay prone, covered in blue drapes. Only an island of skin was exposed just over the wrist. The extensor tendons glistened in the bright operative lights. “Can I get the self-retractor? . . . And some irrigation please?”
Alia continued teasing apart the extensor retinaculum of the fourth compartment. She could sense the weight of Saanen’s piercing green eyes on her hands. He studied each movement as she finally reached the scaphoid capsule. “What do you see, Alia?” She wasn’t used to Saanen calling her by her first name. “Well, I see the dorsal carpal branch of the radial artery here,” she said while pointing it out with her Metzenbaum scissors. “We want to avoid disrupting its capsular attachment to the scaphoid.” Saanen simply handed her the 15-blade scalpel. Alia straightened her back and slid the stool forward an inch. Cutting into the scaphoid capsule, a bead of blood surfaced. The only reminder that this arm belonged to someone still alive.
“So, cashews—” Saanen posited, “those will kill you, right?”
Alia barely lifted her eyes towards Saanen, her attention entirely on the deep dissection to expose the fracture site without accidentally nicking the artery. A few moments later, she finally took a breath in. “It’s not the worst thing that can happen on call,” she murmured.
“I haven’t had anaphylaxis since I was three.”


During one of our group sessions, our mentor and medical school group leader opened up about her personal journey. “Every time I caught a glimpse of it in the mirror, I felt marked, almost branded,” she confided, her voice catching as she spoke directly to us. She explained that the black X drawn on her skin was a functional marker — overlying a tiny, rice-grain sized indicator used by her surgical team to precisely locate the tumor for an upcoming lumpectomy to treat her breast cancer. Even though she was sharing her own experience as a patient, she continued to teach and guide us through that raw, jarring moment — a collision between her clinical expertise and the vulnerability of being on the other side of care.
“I felt dirty,” she told us. “It felt like it was trying to define me. And I hated it.” Her words were a revelation to me that day. They cast a shadow over something I had always viewed as purely clinical: surgical markings. These marks are a routine and necessary step to guide surgeons where to incise, where to reapproximate tissues, and confirm the right body part to be operated on. Surgeon mentors in the past taught me to mark with abandon, as the utility in the OR was on their mind. But her story revealed something I had never considered — that the emotional weight of a mark depends entirely on its context. Hearing from her about the weight of the black ink struck me: How did I not think of this before? Black, a color so often associated with finality and mourning, seemed harsh and unforgiving against the backdrop of her vulnerability. The X, like a wrong answer on an exam, seemed less like a guide and more like a pronouncement — a symbol that marked her body as diseased, as if the cancer itself had inscribed its claim.
For a patient undergoing plastic surgery, markings might symbolize transformation or hope — a carefully laid blueprint for a new beginning. Yet for my mentor, that black X was not a harbinger of change but an unwelcome intrusion, a stark reminder of cancer’s grip on her life. It wasn’t a mark of healing or progress; it was an indictment, a scar before the incision that weighed heavily on her sense of self.
Just as we choose our words with thought and care in medicine to comfort and guide patients, perhaps we should extend that same deliberation to surgical markings. If language, when chosen mindfully, can shape a patient’s experience, then so too might a reimagined approach to these physical marks — transforming them from symbols of disease into signals of hope and healing.
Her story made me think about how we, as future clinicians, might approach these moments differently. The contrast between logically understanding the clinical necessity of the mark and the raw emotion of seeing the mark on her own body brought a new perspective to the patient-physician relationship. Could we frame these marks in a way that emphasizes healing rather than disease? Could we engage patients in conversations about what these symbols mean to them? Perhaps it begins with something as simple as explaining the purpose of the marks in a way that connects them to the larger story of recovery, reframing them as tools of precision and hope rather than reminders of illness. Could we offer patients a choice in the appearance of the markings — the color or shape — giving them a sense of agency in a process that so often feels out of their control? Even temporary marks, like the black X, might feel less alienating if they carried a softer hue or symbolized something empowering rather than stark finality. These small changes could profoundly impact the emotional experience of the patient. By engaging in these conversations, we can ensure that even routine aspects of care honor their humanity.
As I move forward in my medical training, I will carry her story with me. Every time I pick up a skin marker, I will think of her. It’s a reminder that every mark we leave, whether physical or emotional, becomes a part of our patients’ narratives. Our responsibility isn’t just to make those marks with care but to ensure that they signify hope, healing, and humanity.
All identifying information is shared with permission.
This article was originally published by Doximity as an Op-Med on April 21, 2025. It can be read at the following link: https://opmed.doximity.com/articles/her-surgical-mark-was-a-scar-before-the-incision
It was the kind of New England summer where the air clung to the skin, thick and sticky with the heat. The concrete platform baked in the sun, and I had to squint to see the rails vanishing behind a curve in the tracks. A subtle squeal in the distance crescendoed as the train pulled into the station, swiftly followed by the acrid scent of the hot brakes. It was a relief to board and feel the cool air of the conditioned cabin. Amid this environment was my first exposure to Michael Crichton’s “Jurassic Park.” As a teenager commuting into Boston every morning for summer camp, I had picked up a frayed copy of the book for a dollar to keep me company on the train ride. But it didn’t matter how humid it was outside, because from the moment the train started rolling and I began flipping the pages, I was somewhere else entirely.

Outside the window, the world blurred into a rush of green — not just a warm summer green, but a deep, saturated green whose vividness felt ancient and alive. We slipped by stretches of forests, punctuated by marshlands with scattered skeletal trees, their bleached limbs reaching out from the swampy brush. In my mind, suburban Massachusetts gave way to the world of Isla Nublar. “Jurassic Park” was the first book where I was terrified to turn the page, but simultaneously couldn’t stop myself from doing so. It was gripping for how lucidly it folded science into suspense. I honestly half-expected to catch a glimpse of a raptor scurrying between the trees. It just felt so possible . . . and I looked. My eyes kept sneaking off the page and toward the window, searching. That was the power of the writing.
At the time, I didn’t know that Michael Crichton had gone to medical school, or that years before writing “Jurassic Park” in 1990, he had written the original screenplay for “ER” in 1974. A physician-turned-writer, Crichton was well-known for suffusing his medical perspective into the realm of popular culture through novels, TV shows, and of course, films. Years later, when I heard about “The Pitt” — a new medical show tied up in a lawsuit from Crichton’s estate accusing it of being an unauthorized “ER” reboot — and saw a YouTube video from Dr. Mike praising its realism, I was curious. The Crichton connection caught my attention. The praise for its authenticity made me actually watch it. In the midst of relentless studying, it was a refreshing take on the profession and a glimpse into the wards.
“The Pitt” was so different from the usual medical procedurals, the likes of “Grey’s Anatomy,” “Scrubs,” “House MD,” “The Good Doctor,” or “The Resident.” Roshan Sethi, a physician and one of the original writers of “The Resident,” in apt timing, had just given a virtual talk at our medical school’s “Beyond the Hospital” elective where he lamented the limitations of network television: the tidy resolutions, the black and white morality, the crass surgeons, the lawless detectives, and the stereotypical casting. By the time Sethi left, the show was flattened into seductive archetypes that work well with mass audiences — a far cry from the rich nuance and messy challenges of real medicine. But that’s Hollywood, he noted. Hence my surprise when watching “The Pitt.” It felt different because it felt real. There were no soapy romances, no outlandish scenarios, just the daily grit of the physicians, nurses, and even medical students, going through their day treating patients one by one.
I felt that I could walk down the hall to the actual ER and see all the same things in person, albeit certainly not within the same day. “The Pitt” plays like a greatest hits highlight reel, compiling all of the most interesting or dramatic patient cases that a doctor might see over a year’s worth of shifts into each jam-packed hour. In Episode 4, the intern, Dr. Santos, puts a patient with a traumatic chest injury and rib fractures on positive pressure ventilation. On the heels of our respiratory unit, I was literally yelling at the screen, “No, No! He’s going to get a tension pneumothorax!” It’s a classic dramatic take in a medical show, and of course my reflex was prescient. This time, I was in on it. In the first episode, a triathlon athlete comes in with weakness and malaise. My instinct was hyponatremia, but I didn’t quite make the connection to rhabdomyolysis as a more seasoned physician might. When the patient crashes, the attending asks the chief resident, Dr. Collins, for a differential. She suggests drug overdose, electrolytes, long QT, Wolff-Parkinson-White. Hey, I know what these are now! It actually makes sense to me. The team, headed by the attending, Dr. Robby, performs an EKG: widened QRS complexes, peaked T waves. Of course; the diagnosis is hyperkalemia from rhabdomyolysis. Even before they suggested it, I thought to myself, “I would give insulin for this to drive the potassium into the cells.” For the first time, I could watch a medical show as someone on the inside. “The Pitt” stands out, not because it’s perfect, but because it feels grounded and sincere in its depiction of modern emergency medicine. It feels visceral.
The drama is faithful to medicine, for once. Authentic drama is best expressed through the vernacular of insiders, argues David Mamet, a screenwriter and fellow pilot. In his illuminating essay, “The Drama of Flight,” he claims that the best aviation writing is not found in the purple prose of Antoine de Saint-Exupéry, but in flying magazines where “pilots are communicating, in technical language, the drama that took place: . . . difficulties, happenstance or error compounded by laziness, fatigue, ignorance or pride; ignorance beaten out through near-averted tragedy; theory triumphing over fear, or excised through practice.”
Far from being dry, this technical language made up of abbreviation, pauses, omissions, and cadences is allusive, even poetic. Its gestures, silences, and shorthand are charged with meaning, containing the weight of fear, fatigue, pride, and competence in just a few words. As such, it’s deeply expressive for those fluent in it. Mamet made this observation while flying solo over the desert of the western U.S., where long hours listening to air traffic radio chatter revealed a staggeringly intimate drama unfolding between strangers in the sky. A slight inflection from the air traffic controllers could, to those fluent in the language, communicate disapproval, apprehension, or warning. “There was the drama one could detect, in the competence of the commercial and military pilots, the result of endless hours; in the private pilots, the relaxed and often folksy diction and vocabulary of the old-timer, the confusion and, sometimes, the apprehension or fear of the [novice].” To make sense of this radio play, he argues, you just have to be able to speak the language.
That same attitude toward the language of medicine is embodied by “The Pitt.” Doctors across America feel heard, going so far as to say: “That’s exactly what happens. That’s exactly what that looks like. That’s exactly the words that I would say if I were in that situation.” In this case, the realism isn’t just a gimmick. Rather, realism is what allows the drama that is inherent to the profession to be teased out, dissected, and laid bare on the table. This fidelity to the real world, including the one-to-one timeline, is purposeful. In a conversation on “The Nocturnists” podcast, Joe Sachs — one of the show’s principal writers and a practicing emergency medicine physician himself — discusses his writing process. The medical cases are chosen specifically to serve the story, they get us to “learn more about the characters and their relationships with each other,” and I might add, to Mamet’s point, the characters’ relationships with themselves. That narrative approach to authenticity is key. The job of the writer isn’t to devise increasingly elaborate scenarios, but to identify which clinical cases naturally allow for character growth. It resonates with those in medicine because we’ve seen those very cases shape who we are, too.
Sachs offers a great example, in Episode 7, where a patient with autism presents with an ankle sprain. This case wasn’t included because the world needs more awareness about ankle injuries, but because it gave Mel, a second-year resident, an opportunity to contrast with other characters. As Sachs explains, her character needed a chance to “show her incredible skills at patient care and compassion . . . as opposed to Langdon, who had no patience, no time, and was doing everything wrong.” The accurate clinical reasoning — her differential including dancer’s fracture vs. Jones fracture and their respective abilities to heal — wasn’t just about being technically correct. It reflected Mel’s ability to hear the patient’s story, ask thoughtful questions, and correctly make sense of the clinical picture with both curiosity and care. The case highlights Mel’s character as an empathetic physician, one who could get “through to the patient in a way that Langdon never could.” What resonates with physicians is how vividly the show captures the real world journey of growth. The character development that unfolds over years of medical training are distilled into moments that feel honest and earned, mirroring our own experiences with the same richness.
“The Pitt” doesn’t explain itself; it doesn’t translate the medicine for the viewer’s benefit. It dares to use the real language of medicine, the technical jargon. Perhaps “The Pitt” feels so real to me because this time I finally know the language; I’m an insider. I’m not quite fluent, but I can certainly understand the basics. Like any modern show wanting to be in vogue, “The Pitt” still has the occasional heavy-handed moral didactics and social commentary. However, the show insists that good drama can be found even in faithful narratives about patient care. The showrunners consciously chose to avoid the sultry charm of McDreamy, the Sherlock-level sleuthing of House, or the absurdist caricatures and meta-commentary of J.D.’s lampooning satire, and chose to engage with us in the bona fide language of medicine; the one that we speak among one another.
To those working in the emergency department, it’s the first show that they can point to and say to their friends and family, “that’s what it’s like at work.” For Joe Sachs, that kind of reaction is personal validation. As he puts it, other physicians have said: “For years, I’ve tried to tell my friends, my family, my significant others, what it’s like to work a shift, and I’ve never been able to put it into words before, and I never have been able to give a sense of what it’s really like. And now that the show’s on the air, they can watch it, and I can say, ’Yes, that’s what I do.’” Of course, “The Pitt” isn’t 100% accurate — no show is willing to depict the sheer number of hours physicians spend staring at a computer screen. Cinema is, after all, meant to explore a heightened sense of reality. Audiences still want to see more of the “old-school heroics” of medicine — sans all of the note-writing — and we still want to be entertained.
What’s striking is that it still works for people outside medicine. The show doesn’t pause to decode its terms or slow down for melodramatic story beats. It trusts that the layperson will catch the rhythm, if not the exact content, and sense the stakes in the tone, the urgency, and the chaotic choreography of people moving through clinically lit set pieces. In essence, it’s a sneak peek into the hermetic environment of the modern emergency room, with all the same real stakes. The show suggests that perhaps what audiences crave in modern medical shows isn’t sensationalism or soapy romantic sagas — it’s competence. In a cultural moment when trust in institutions has faltered, audiences revel in watching professionals speak fluently and act decisively to save lives. That’s what “The Pitt” gets right.
This article was originally published by Doximity as an Op-Med on August 28, 2025. It can be read at the following link: https://opmed.doximity.com/articles/when-the-drama-of-medicine-speaks-for-itself


It sat on my shelf, creased just-so, the slim spine a reminder of what I thought medicine could be — a journey of discovery, resilience, and learning the skill of managing uncertainty. My professor gifted it to me, a nod of encouragement for my journey as both a medical student and a writer: Siddhartha Mukherjee’s The Laws of Medicine. One passage from the book has lingered in my mind, depicting a legendary surgeon, Dr. Castle, whose presence in the OR was nothing short of commanding. His mastery of surgery, so formidable “that he allowed the students to do most of the operating, knowing that he could anticipate their mistakes or correct them swiftly after,” left an indelible mark on those around him. And then, as if to hint at his humanity outside the OR, Mukherjee snuck in a one-sentence mention of Castle’s weekend retreats to the sea, where he sailed on a vessel aptly named “The Knife.”
On the top of the same bookshelf sat a model of the 1992 America3 sailing yacht, its mast just barely avoided scraping the ceiling. It, unlike the book, was indeed a mere trinket; ornamental as a means to suggest refinement of taste. Years later, I thought back to these bookshelf items while watching the sailboats on the lake from the seventh-floor conference room of my medical school. From that vantage point, I observed the sailors, occasionally glimpsing moments of struggle as they grappled with the lines, trying to tame the luffing sail. It felt like a serendipitous sign.
The imagery of Dr. Castle, both in the OR and his leisure time on the water, fascinated me. This was the archetypal surgeon: skilled, composed, and confident in every facet of his life. It wasn’t long before the seed planted by the story of Dr. Castle took root in my mind. I found myself drawn to the sailing club on the lake, perhaps yearning to give reason to the model yacht holding such a prominent position in my room, or perhaps conflating my desire to be the man written on the pages with the need to be a sailor. Either way, and on a whim, I made the decision to sign up for sailing classes during the summer of medical school.
As I stepped onto the deck of a sailboat for the first time, a sense of apprehension quickly enveloped me; my sense of stability rocked with each small wave. The terminology was entirely foreign – “it’s time to raise the halyard,” “don’t forget to tighten the boom vang,” or “we’re not ready to gybe yet” – but beneath the surface lay an undeniable allure: a promise of childlike adventure, a chance to learn something new without the responsibility to be good at it yet. A fitting promise, as our adult class followed a summer camp of nine- and ten-year olds learning the same things earlier in the day.

In the weeks that followed, I immersed myself in the world of sailing, learning the ropes — quite literally — and embracing the process of learning with a childlike curiosity that I hadn’t felt in years. Sailing was entirely new to me, and with that unfamiliarity came a refreshing sense of freedom. There was no pressure to be an expert or even to be competent — just the joy of discovery. Much like the children in the camp immediately before us, I allowed myself to stumble, make mistakes, and, more importantly, ask questions without inhibition.
When I took that spirit of learning back to medical training, that same sense of awe and wonder became readily apparent in my studies. I found a renewed motivation to push through the challenges and rigors of medical school. As adults, we often shy away from admitting what we don’t know, fearing judgment or embarrassment. This is especially true in medical school. But in this new setting, surrounded by knots, sails, and terminology that made little sense to me at first, I let go. I was no longer concerned with how I appeared to my peers. I tapped into the openness of my inner nine-year-old, who wasn’t afraid to ask why the boom vang needed tightening, what would happen if the sail wasn’t properly trimmed, or, for the 12th time, what the clew was.
In doing so, I rediscovered the beauty of learning like a kid — not burdened by the self-consciousness of adulthood, but driven by an insatiable curiosity. Every mistake was a lesson, every failure an opportunity to understand something new. Like the children who spent their summer mornings mastering the art of tacking and gybing, I approached each challenge with a willingness to fail, eager to see what the next lesson would teach me. In the seriousness of medicine, it’s a lesson that I often neglected.
Learning in this way also brought an unexpected joy. I found myself laughing at my missteps (and almost falling in the water at least once), celebrating small victories like tying a proper knot or gybing without losing control of the boat. With each outing, my skills grew, but more importantly, so did my sense of wonder and appreciation for the learning process itself. That summer of sailing, it turns out, was not just about mastering technique — it was about recapturing the fearless, inquisitive spirit of youth. Bringing that same fearless curiosity back to medical school, I’m reminded that the path to becoming a doctor isn’t just about getting things right; it’s about embracing each challenge as an opportunity to learn and grow, with the wonder and excitement of a child.

This article was originally published by Doximity as an Op-Med on January 21, 2025. It can be read at the following link: https://opmed.doximity.com/articles/learning-the-ropes-of-medicine-literally
This article was reprinted in the Spring 2025 issue of Worcester Medicine. It can be read at the following link: https://issuu.com/wdms/docs/worcestermedicine-spring2025_
Years ago, as a medical student in Boston, I watched a senior surgeon operate on a woman. The surgeon, call him Dr. Castle, was a legend among the surgical residents. About six feet tall, with an imposing, formal manner that made the trainees quake in their clogs, he spoke in a slow, nasal tone that carried the distinct drawl of the South. There was something tensile in his build—more steel wire than iron girder—as if his physique had been built to illustrate the difference between stamina and strength. He began rounds at five every morning, then moved down to the operating theaters in the basement by six fifteen, and worked through the day into the early evening. He spent the weekends sailing near Scituate in a one-mast sloop that he had nicknamed The Knife.
The residents worshiped Castle, not only for the precision of his technique, but also the of the quality of his teaching. Other surgeons may have been kinder, gentler instructors, but the key to castles teaching method was supreme self-confidence. He was so technically adept at surgery—so masterful at his craft—that he allowed the students to do most of the operating, knowing that he could anticipate their mistakes or correct them swiftly after. If a resident nicked an artery during an operation, a lesser surgeon might step in nervously to seal the bleeding vessel. Castle would step back and fold his arms, look quizzically at the resident, and wait for him or her to react. If the stitch came too late, Castle’s hand would reach out, with the speed and precision of a falcon’s talon, to pinch off the bleeding vessel, and he would stitch it himself, shaking his head, as if mumbling to himself, “Too little, too late.” I have never seen senior residents in surgery, grown men and women, with six or eight years of operating experience, so deflated by the swaying of a human head.
Siddhartha Mukherjee, “The Laws of Medicine”


The afternoon air had a palpable starchiness to it, cool and damp but still thick. As I arrived at the airport around 3 p.m., a bright haze lingered in the sky. Only a few other people were present as my brother and I walked towards the hangar: a flight instructor and her student debriefing from their lesson, another pilot shuffling around his plane filling the fuel tanks, and 5 or 6 other planes sitting parked, scattered along the ramp. Inside the hangar, the afternoon light streamed in through the gaps of the corrugated metal construction. The rusty wheels groaned in protest as the large hangar door raised, their grating screech reminiscent of nails on a chalkboard. With the door open to the beautiful vista outside, I set my bag on the floor and pulled out the checklist. Stained blue from the occasional drips of aviation fuel, this small piece of paper was my Bible.
My training as a pilot means that I’ve become an ardent supporter of checklists, and I hope, an effective user of them. As a medical student, I’ve had the privilege of observing many different surgical teams, and while my experience in the OR is still growing, my background as a pilot has given me a unique perspective on the value of checklists. I’ve noticed that in medicine, some of my colleagues seem to suffer from checklist fatigue – a very real challenge that I believe stems from a misunderstanding of what checklists are truly meant to accomplish. The purpose of my checklist as a pilot is to: (1) help correctly configure the aircraft, consistently; (2) mitigate human factors by assuming humans are imperfect; and (3) prompt the pilot to brief the tasks that do require adaptability and judgment.
These days, I walk around the plane scanning the leading edge of the wing with my eyes and running my hand over the rivets and screws that hold it together, often without ever glancing at the physical paper. I’ve gotten so used to the flow of my pre-flight checks that I don’t need anything to remind myself what to do. However, it was hammered into me as a student pilot that mental flows like this should always be backed up with the physical checklist — just in case. It’s become a habit now, that after the exterior pre-flight, I pause and read each item in my checklist out loud. Crucially, as I read each item aloud, I actively recall inspecting it.
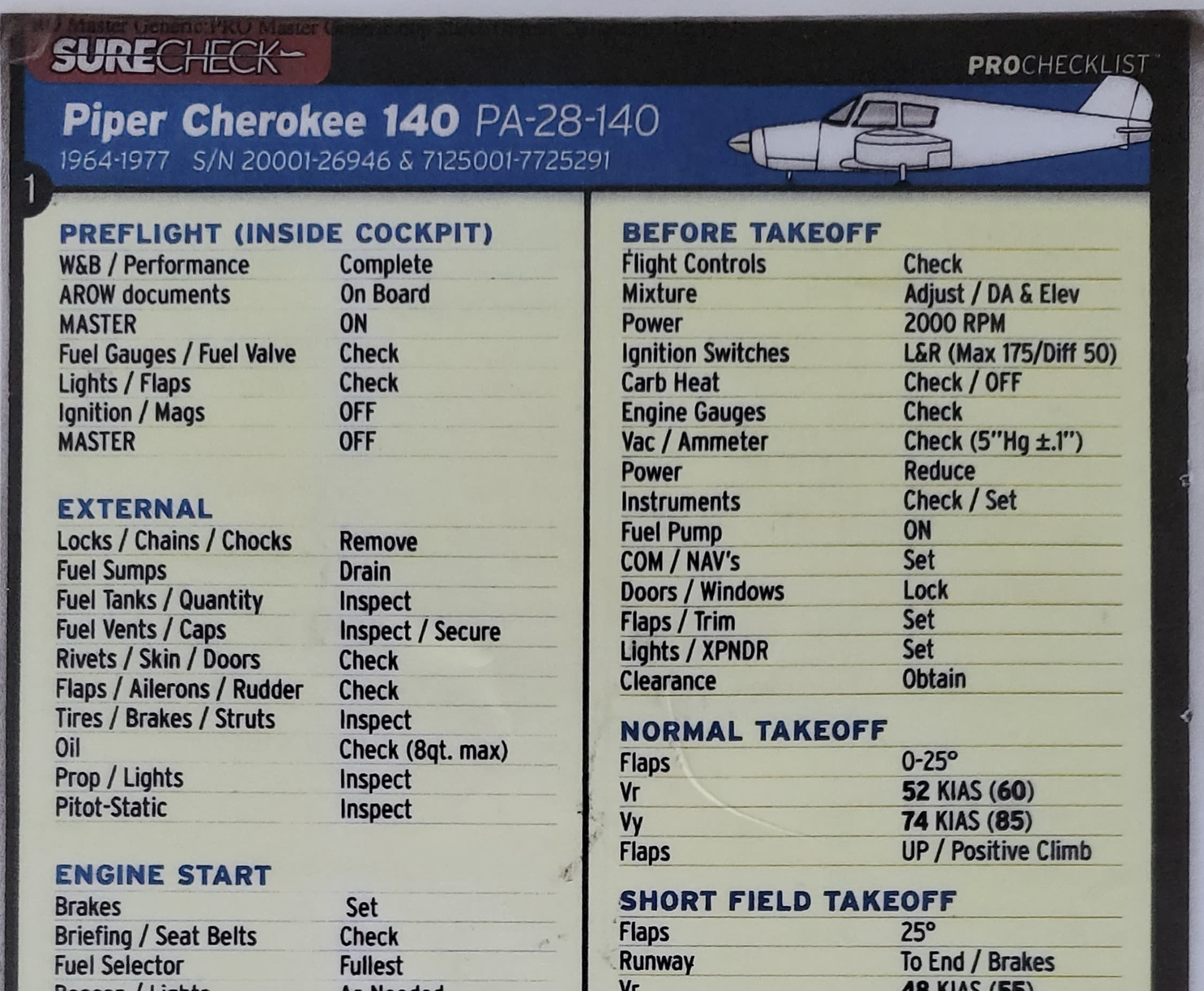
For example, one of the lines reads: “Tires / Brakes / Struts.” It’s easy to simply read it off rotely, without fully being aware that you’ve checked each separate item. I’m certainly guilty of this too. Now, as a more experienced pilot, I realize that doing so is a disservice to myself, my passengers, the people on the ground without any control of the matter, and all those who place their trust in us as pilots.
On that cool afternoon day, as I read that line, I thought to myself:
- “Did I press hard on the tire to feel its pressure and rebound?” I remembered pushing down on the tire and looking at the treads and seeing that, while the front tire was well-worn, it would suffice for a few more months before needing replacement.
- “Did I move the wheel ever so slightly to see the gap between the brake pads and the rotor?” I remembered looking at the pads and the rotor, not seeing any grooves from contaminants that might have gotten lodged in between.
- “Did I look at the struts to see that there was plenty of space for suspension travel?” I remembered seeing the characteristic wear of the strut sliding up and down, absorbing all of the previous landings. It was clearly not bottoming out its range of motion.
This mental exercise took altogether less than a second. It’s a backup that gives me a chance to correct a deficiency while still on the ground. It’s a reminder that the checklist is not the physical piece of paper, but instead it is the act of actively recalling that each item was inspected or set correctly. I fully believe that this attitude contributes greatly to my safety in the air.
The same applies for medicine. Checklists must be specific; to each procedure, or at least specific to the specialty. Checklists must be sparse, only including the most critical elements that cannot be missed. Checklists should prompt the team to dig deeper where required, such as for particular procedures that need certain post-operative considerations or pose a greater risk of a sharps mishap. Checklists must encourage the team to brief the complexities where judgment is necessary. And perhaps most importantly, teams should be trained to use checklists effectively, starting with the pilot-in-command: the surgeon.
My hope is that when you come across a bad checklist, you can take charge to customize the checklist to work for you. Perhaps you can remove unnecessary items, or adjust the verbiage to say “Imaging available / As needed” instead of a yes/no checkbox, or create different checklists that include imaging only in procedures that actually require it. The success of my flights has reinforced my attitude toward checklists: I see them as tools for ensuring consistency, safety, and clarity, not as burdens or boxes to check. This mindset allows me to embrace their purpose and see beyond their limitations. With a well-designed checklist, and the right mindset, you’re not just following a procedure; you’re enhancing your ability to provide the best care possible in all situations.
While checklists are invaluable for ensuring consistency and covering critical elements, they are only part of the equation. Equally important is the role of briefings, which complement checklists by allowing space for the nuances and complexities that require professional judgment. I want to emphasize an important distinction in terminology. A “briefing” is different from a “checklist.” A checklist might prompt you to do a briefing, but the briefing enables you to consider the specifics of the particular scenario. It allows you to bring in that clinical judgment that can be lacking in surgical checklists. For example, as I’m sitting at the threshold of the runway, my pre-departure briefing prompts me to consider what obstacles will be ahead, what radio frequencies I will use to communicate to air traffic control, and what heading we will need to fly to get on course toward the destination. I think through the specifics that aren’t accounted for in a checklist.
This approach isn’t limited to the cockpit. Whether managing a flight or diagnosing a patient, the discipline of checking everything thoroughly – and questioning anything that seems off – is crucial. In both fields, safety and success depend on recognizing that the checklist is an essential tool, but not a substitute for critical thinking, human judgment, or intuition.
The checklist is more than just a series of rote tasks; it’s a physical manifestation of a core philosophy in aviation: humans are not infallible. Aviation embraces a systematic approach that acknowledges our human limitations and proactively builds in safeguards to reduce errors. Whether it’s a checklist, a pre-departure briefing, or simply reading things aloud, these are simple tools that help me fly safely. This philosophy recognizes that no matter how experienced we are, we all have blind spots and moments of complacency. By transferring this mindset to medicine, where the stakes are equally high, we can create systems that support clinical judgment, prevent oversights, and ultimately improve patient outcomes. Embracing the aviation approach in medicine means accepting that even experts need checklists, and that doing so is a strength, not a weakness.
This article was originally published by Doximity as an Op-Med on November 4, 2024. It can be read at the following link: https://opmed.doximity.com/articles/pilots-love-checklists-so-why-don-t-surgeons
My brother and I decided to fly up to Laconia, New Hampshire, near the beautiful Lake Winnipesaukee to explore the area. We’re hoping to fly to Alton Bay, an ice runway that opens up every year once the ice is thick enough, as it’s only a 10 minute flight from Laconia. Prudent aeronautical decision making means that we wanted to go explore the area first so were familiar with it before attempting a much more challenging trip!
Part of a Series: Reflections from Medical School
The evening sun spilled through the leaves of the oak tree, illuminating the parking lot of the church with dancing shadows. The shade provided some refuge from the summer warmth. This exquisite lighting framed our arrival as if it were a movie. My brother and I walked past a lineup of cars, waiting to check in for their appointment at the free clinic. In front of us walked another volunteer who had arrived only a minute before us.
Amidst the line was a small, blue Mercedes SUV with the windows open. Probably a GLC 300. A family sat inside, waiting quietly for a clipboard-brandishing volunteer to help check them in. Instead, the volunteer walking in front of us, who had not even entered the clinic yet, literally stopped in her tracks, mouth agape. She waved her arm furiously, clear disappointment coursed through her voice. “A Mercedes at a free clinic!?”
As we entered the building, waiting for our temperature to be checked, she repeated the sentiment to me. Incredulous, I initially thought she was joking. I was shocked that a volunteer at a free clinic would so openly and vehemently say something like this. Quickly it became apparent that she genuinely thought that any person in a Mercedes shouldn’t be coming to a free clinic. I didn’t want to argue, but I did tell her that I strongly disagree with that. Perhaps the patient lost their job and no longer has health insurance (a common issue, unfortunately)? Perhaps they are bringing an elder who is visiting from a foreign country?
I thought back to an article in the Washington Post which was strikingly similar, describing the experience of getting food stamps in a Mercedes. Either way, however, it is completely inappropriate to say something like this at a free clinic, much less within earshot of the patient.
We bought a house. Then, just three weeks after we closed, the market crashed. The house we’d paid $240,000 for was suddenly worth $150,000. It was okay, though — we were still making enough money to cover the exorbitant mortgage payments. Then we weren’t.
Two weeks before my children were born, my future husband found himself staring at a pink slip. The days of unemployment turned into weeks, months, and, eventually, years.
Then my kids were born, six weeks early. They were just three pounds each at birth, barely the length of my shoe. We fed them through a little tube we attached to our pinky fingers because their mouths weren’t strong enough to suckle. We spent 10 days in the hospital waiting for them to increase in size. They never did. Try as I might, I couldn’t get my babies to put on weight. With their lives at risk, I switched from breast milk to formula, at about $15 a can. We went through dozens a week.
In just two months, we’d gone from making a combined $120,000 a year to making just $25,000 and leeching out funds to a mortgage we couldn’t afford. Our savings dwindled, then disappeared.
Darlene Cunha
I was utterly shocked that someone could judge someone and have that much prejudice against a Mercedes when they’re volunteering in a free clinic.
“Sell the Mercedes,” a friend said to me. “He doesn’t get to keep his toys now.”
But it wasn’t a toy — it was paid off. My husband bought that car in full long before we met. Were we supposed to trade it in for a crappier car we’d have to make payments on? Only to have that less reliable car break down on us?
And even if we had wanted to do that, here’s what people don’t understand: The reality of poverty can spring quickly while the psychological effects take longer to surface. When you lose a job, your first thought isn’t, “Oh my God, I’m poor. I’d better sell all my nice stuff!” It’s “I need another job. Now.” When you’re scrambling, you hang on to the things that work, that bring you some comfort. That Mercedes was the one reliable, trustworthy thing in our lives.
That’s how I found myself, one dreary day when my Honda wouldn’t start, in my husband’s Mercedes at the WIC office. I parked gingerly over one of the many potholes, shut off the purring engine and locked it, then walked briskly to the door — head held high and not looking in either direction.
To this day, it is the single most embarrassing thing I’ve ever done.
Darlene Cunha
It’s already difficult enough to bring yourself to come to a free clinic. Patient’s judge themselves harshly, thinking that this is not a resource that they should need. As a result, it’s critical that we make the environment a safe space for patients so that everyone can feel welcomed.
Dossier
“This is what happened when I drove my Mercedes to pick up food stamps,” by Darlena Cunha, July 8, 2014. https://www.washingtonpost.com/posteverything/wp/2014/07/08/this-is-what-happened-when-i-drove-my-mercedes-to-pick-up-food-stamps/
There are so many interesting airports scattered throughout the state of Massachusetts. One that I’ve wanted to visit for a long time is Marshfield, just off of the coast and south of Boston. The fun part of this flight is flying from Fitchburg, and going underneath the busy airspace of Boston’s Class B airspace and through the Norwood Class D airspace. The views were stunning too!
Coming back from a flight, the last thing we do is land the plane! While it’s not all that complicated, it does take a lot of practice and skill to do land smoothly. Here, I go through what I think through as I land — all in real time. Keep in mind, I am not a flight instructor. This is based on my own personal experience as a pilot, so take it with a grain of salt!